
Fiona has a rare cancer and feels that the best way to combat her feelings of acute anxiety is to get back in control by doing in-depth research on the internet. She prints out a sheaf of papers to take to her consultant
Samuel believes that he is being over-treated for hypertension. He buys a good quality blood pressure monitor so that he can do his own testing at home.
Susanne has a common heart condition, which she monitors through sensors and an app on her smartphone. This alerts her to the need to get urgent medical help if her condition deteriorates.
Will Fiona’s consultant welcome her research or will he patronise her by saying dismissively, ‘Oh leave me to worry about that!’? Will Samuel’s GP insist that her own surgery-based measurements are the ‘right’ ones, or see that she has a co-operative patient, eager to manage his own health? Will Susanne’s cardiologist feel relieved or worried that he has a patient so actively involved in her own care?
My co-author, Dr Arti Maini, and I became intrigued by the whole question of how clinicians could use a coaching approach in their daily work with patients, which we then explored in our book Coaching for Health: Why it Works and How to Do it.1 Arti is a GP and coach and I am an executive coach. We had worked together on an innovative project for the London Postgraduate Medical School and had seen for ourselves when training hundreds of clinicians, mostly doctors and dentists, how radical the transformation could be when our participants understood the potential for coaching rather than instructing or rescuing their patients.
All effective coaching accepts that the human approach to change is ambivalent: the bigger the change, the more reluctant we human beings are to make it. This is the opposite of the implicit assumption in so much clinical training, which is that all you have to do is to inform people about what is good for them, using all the authority of your role, and they will obediently do it.
Why ‘telling’ doesn’t work
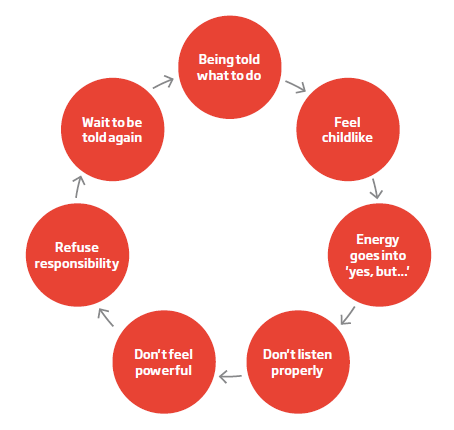
When another human being insists by telling, ordering and directing, our typical response is to resist. The amygdala in the brain experiences it as an attack, so our higher thinking processes shut down. We may fight back with arguing or physical resistance, or else we feel undermined and childlike. Our attention goes to proving the other person wrong: ‘Yes, but…’ is often the immediate response.
This will be true even when the person doing the telling is someone we respect. What will typically happen is that we nod politely, so resistance may not be visible. But inside, we may feel disappointed – with ourselves for not speaking up, or with the other person for not listening. Or we may feel angry that the other person made such unwarranted assumptions about us when a few questions might have revealed our real worries and concerns.
What patients actually do with the advice that clinicians give them
You will most likely know of stories like these which suggest that change is needed:
After Jim died, his sister discovered five bulging plastic bags under his bed. They contained the medication he had been prescribed over the years of his illness. He had dutifully collected all his drugs but had taken none.
Ted knows he has osteoporosis. He has filled in a lifestyle questionnaire and the doctor glances at it. Then she launches into a little talk on nutrition, including the importance of limiting alcohol and consuming enough calcium and oily fish. Ted half-listens, too annoyed to tell her that although officially retired, he is still an internationally recognised expert on nutrition and probably knows more than she does about the nuances of diet in osteoporosis.
Cynthia has just seen the diabetes specialist nurse. She was told that she is 15 kilos over her ideal weight and that she has a BMI (body mass index) of 35. She nodded politely but she doesn’t know how kilos compare with stones and pounds, or what BMI means.
These anecdotes illustrate what we already know from research.2 Half of patients leave visits to primary care not having understood what their doctor or nurse has told them. Although it is well established that shared decision making improves outcomes, only nine per cent of patients say they participated in decisions about their health. Average adherence rates for prescribed medications are around 50 per cent: one recent survey estimated that £300 million was wasted in England alone on medication that was ordered from the pharmacy but never taken or finished. When clinicians suggest lifestyle changes to reduce the impact of illness, only 10 per cent of patients follow their advice.2
Patients are less patient
As patients, we are far less likely to be docile than was once the case. We are better educated, with more confidence and willingness to challenge. There is less automatic respect for authority; it has to be earned and depends more on moral authority than on hierarchical position. Then there is the complementary health phenomenon: we want someone who will listen with warmth, give us time, take us seriously, treat us as equals. Interest in these approaches may in part represent a frustration with how we experience mainstream healthcare.
The impact of health ‘scandals’
Media exposures of unethical and disrespectful clinical practice have played their part in damaging automatic deference to the clinical professions. We are more willing to comment in public about health encounters, whether through a well-considered blog or through impulsive posts on Twitter. We are more impatient with waiting; we are less tolerant of behaviour in clinicians which could be seen as incompetent, poorly communicated, discourteous or dismissive. It is also much simpler to complain than it ever has been in the past: where a complaint might previously have been dismissed for lack of evidence, nowadays some patients can and will make secret recordings to boost their case.
Clinician stress
These changes have created new challenges for clinicians, most of whom feel an immense sense of responsibility for the patient’s wellbeing: it is why they went into the clinical professions in the first place. If this gets out of control, they can feel that they are never good enough, leading to high levels of stress. Fear of complaints can lead clinicians to more ‘defensive’ practice, such as unnecessary referrals and unnecessary prescribing.
The well-known neurosurgeon, Henry Marsh, published his book, 'Do No Harm',3 to some astonishment from fellow doctors at his candour. The book describes the impossibility of offering long-term cures, the multiple quiet triumphs, along with the occasional devastating failures. He describes his rapid descent into fear when he receives a letter from a solicitor threatening a lawsuit:
‘... I feel as though I am about to fall into a frightening world where the usual roles are reversed – a world in which I am powerless and at the mercy of patients who are guided by suave, invulnerable lawyers who, to confuse me even further, are dressed in respectable suits just as I am and speak in the same self-confident tones. I feel that I have lost all credibility and authority that I wear like an armour when I do my round on the wards or when I open a patient’s head in the operating theatre’ (p158).3
Demographic change has added to the challenge for clinicians. The number of people with long-term conditions such as diabetes, cardiovascular disease, depression and arthritis is steeply increasing. These conditions absorb 70 per cent of the health budget.2 Poor lifestyle choices mean that there are rising numbers of people with preventable conditions caused by obesity, smoking, lack of exercise or alcohol misuse. There is a sensible expectation that clinicians can or should be able to play a part in prevention and control here: an ideal scenario for health coaching.
Defining health coaching
Here is the definition we use in our book:1
‘Health coaching is the art of facilitating the patient’s active participation in managing their own health. Coaching raises self-awareness and identifies choices. Through using a coaching approach, patients are able to find their own solutions to enhancing health-related quality of life.’
Six principles of health coaching
This approach is based on six foundation principles of coaching, adapted from the 4th edition of my book, Coaching Skills: The Definitive Guide to Being a Coach.4
- Patients are resourceful
- The practitioner’s role is to move from expert to enabler
- It is best to take a whole-life approach
- The patient brings the agenda for the consultation
- Practitioner and patient are equals in the consultation
- Coaching is about change and action.
These principles imply something far more radical than other common approaches to ‘patient empowerment’/‘activation’ or ‘choice’. They assert that patients have the capacity to be resourceful, even when they seem passive or anxious, acknowledging that the patient is the one who is responsible for their health and knows him or herself better than any clinician can. Taking a whole-life approach means that the other issues in patients’ lives will have the power to enhance or hinder whatever is going on with their health. When you accept that it is the patient who brings the agenda, you are acknowledging their need for autonomy. Assuming that you are equals in the consultation implies mutual respect, listening as much as talking and holding back from early interrupting, rather than having preconceived ideas about where the conversation should go. Honouring the principle of change means that the expected result of the conversation is that something will change for the better. If the patient does not wish to change, or cannot for some reason, then coaching is not the right approach.
What’s the evidence that it works?
There are growing data on the benefits of health coaching. The Evidence Centre has published a review of the current evidence,5 which highlights that the methodology is often not robust and that there is limited research on long-term effects. The studies are difficult to compare with each other for a host of reasons, including large variations in the definitions of health coaching, methods of delivery and types of professional delivering it, and also variations in patient populations. There are also inconsistencies in the competencies and levels of training of the people providing the services.
Benefits for patients
The research community has been taking steps to address these issues. The findings from some recent studies are encouraging. For example, 800 healthcare professionals, drawn from 31 organisations across the East of England, were trained in health coaching skills from April 2013 to October 2014. An interim report has described patient and financial benefits, which included ‘reduced tests and activity resulting from more effective consultations; improved health behaviours; improved patient motivation to self-care; patients setting self-determined goals; improved medication compliance; developing shared responsibility and improved health’.6 Duke Integrative Medicine, based in the US, is leading research, including randomised controlled clinical trials,7 on health coaching for long-term conditions such as diabetes and cardiovascular disease.
Benefits for clinicians
The evidence for benefits to clinicians is still emerging, but so far it seems that these are as powerful as they are for patients. The clinicians Arti and I have trained consistently report greater satisfaction with their work, reduced stress and fewer patients who appear to be impossible to help. These clinicians are able to distinguish the occasions when it is essential to take responsibility for the patient and the majority of times when it is not – and releasing yourself from inappropriate responsibility immediately reduces stress. In our experience, such clinicians are also far less likely to be the focus of complaints. Coaching can transform the way doctors see their work, as these two GPs report:
"I no longer have ‘difficult’ patients since I started using a coaching approach, I feel more in control of the consultation, more aware that I can’t do everything and a lot less stressed.
"Previously, I often ended the day feeling as helpless as many of my patients. It’s forced me to examine a lot of my assumptions about what patients could and couldn’t do or understand. It feels like a shared responsibility, whereas previously it felt like it was all down to me."
Why health coaching works
Coaching works in a health context for exactly the same reasons that it does elsewhere. By assuming that the patient is resourceful, it taps into the patient’s resourcefulness. By assuming that the patient is the one who knows him/herself best and who must live with the results of any treatment, it puts a premium on empathy, on careful listening and on respect for patient choices. By doing this, it increases the chances that the most important problems will be dealt with swiftly, thus reducing attendance at GP and outpatient clinics.
All clinical management is about change: as patients, we want something to be different: to feel less depressed, to have better pain management, to be reassured, to choose the right option for surgery, to get the correct medication for whatever is wrong – and so on. But change is not a simple process. We may want the eventual outcomes of the change and yet resist the path to getting there.
To help patients make beneficial change, it is essential to understand why as patients we may not accept the information we are given, why we may resist being given advice. Clinicians need to know what to do instead and why coaching can so often be the approach of choice.
My own GP seems to be a convert. Consulting her about a minor but puzzling skin condition, she starts the dialogue by asking me, ‘What’s our goal for this consultation?’ This is the first time any doctor has ever asked me this vital coaching question. Then she assumes, rightly, that I will have consulted Dr Google and will have taken some pictures on my smartphone, and she asks me for my opinion. Wow! Puts me on the spot in the best possible way. Then, together, we discuss what might work. Brilliant!
Figures first published in Rogers J, Maini A. Coaching for health: why it works and how to do it © 2016. Reproduced with the kind permission of Open International Publishing Ltd. All rights reserved.
Figure 1.1: Insistence creates resistance 1
We believe what we hear ourselves say
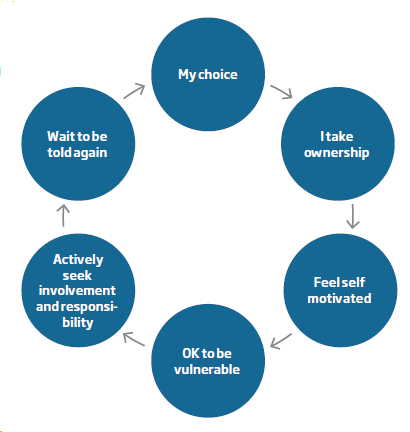
The coaching approach is based on evidence that we believe what we hear ourselves say. When we make our own choices, we take ownership of them, we are self-motivated, feel empowered, offer our own ideas and solutions and are far more likely to put them into action.
Figure 1.2 Choice creates empowerment 1
When encouraged to think for ourselves in response to challenging questions framed empathetically, it becomes more difficult to go on droning through the same old answers. The right questions dismantle resistance and uncover a different and better quality of data. A coaching approach to health assumes that because the patient is the one who will implement decisions and live with the results, the art for the clinician is in asking the right questions and offering information in the right way, rather than in telling people what to do. There are innumerable other reasons for believing that coaching for health is an approach whose time has come.
Jenny Rogers is an executive coach, writer and supervisor. Her book, Coaching Skills: The Definitive Guide to Being a Coach, has become the standard reference text worldwide. She has written books on the MBTI and the FIRO-B and is Series Editor of 'Coaching in Practice', from the Open University Press.
More from Coaching Today

The sports coach meets the executive coach: what can we learn from sports coaching?
Open article: In the first of this two-part series, Erik de Haan and Pat McCarry review the role of the contemporary, elite sports coach and consider the skills that might be realistically applied to coaching in other contexts. Coaching Today, October 2016
Why I became a coach: Depth and breadth
Open article: Executive coach and BACP Coaching Executive member Michèle Down describes her own journey into coaching. Coaching Today, July 2016

Facilitators of integration: finding a place of zero
Open article: Margaret Chapman-Clarke explains why counsellors who coach are ‘conscious change agents’ and can help clients reach a ‘place of zero’ in a volatile, uncertain, complex and ambiguous (VUCA) world. Coaching Today, April 2016
References
1 Rogers J, Maini A. Coaching for health: why it works and how to do it. Maidenhead: Open University Press McGraw Hill Education; 2016.
2 World Health Organization. Adherence to long term therapies: evidence for action, 2003. [Online.] www.who.int/chp/knowledge/publications/adherence_report/en/2003.
3 Marsh H. Do no harm. London: Orion Publishing Group; 2014.
4 Rogers J. Coaching skills: the definitive guide to being a coach. London: Open University Press McGraw Hill Education; 2016.
5 NHS Health Education East of England. Does health coaching work? Summary of key themes from a rapid review of empirical evidence. April 2014 [Online.] https://eoeleadership.hee.nhs.uk/sites/default/filesDoes%20health%20coaching%20work%20-%20a%20review%20of%20empirical%20evidence_0.pdf
6 NHS Health Education East of England. Health coaching for behaviour change: better conversations, better care. Interim Progress Report. June 2014. [Online.] https://eoeleadership.hee.nhs.uk/sites/default/files/1404813191_LmkH_health_coaching_interim_progress_report.pdf
7 Ratanawongsa N, Korthuis PT, Saha S, Roter D, Moore RD, Sharp VL, Beach MC. Clinician stress and patient–clinician communication in HIV care. Journal of General Internal Medicine 2012; 27(12): 1635–1642.
8 Duke Integrative Medicine. Research. http://www.dukeintegrativemedicine.org/research