There is a mental health crisis occurring within the autistic population, which counsellor training and practice is widely unaware of, and therefore not currently equipped to tackle. We have the power to help to change this, but to change, we must be aware there is a problem in the first place. After all, knowledge is power.
Figure 1 below makes for stark reading. The chart highlights the prevalence of some of the serious mental health concerns experienced by autistic people, compared with the same concerns experienced by the neurotypical (non-autistic) population.
Figure 1. A comparison chart of co-morbid conditions and behaviours commonly found in people with autism, alongside the same conditions and behaviours found in the neurotypical population.1 Reproduced from The Neurodiversity Reader 2020, with the permission of Pavilion Publishing and Media.
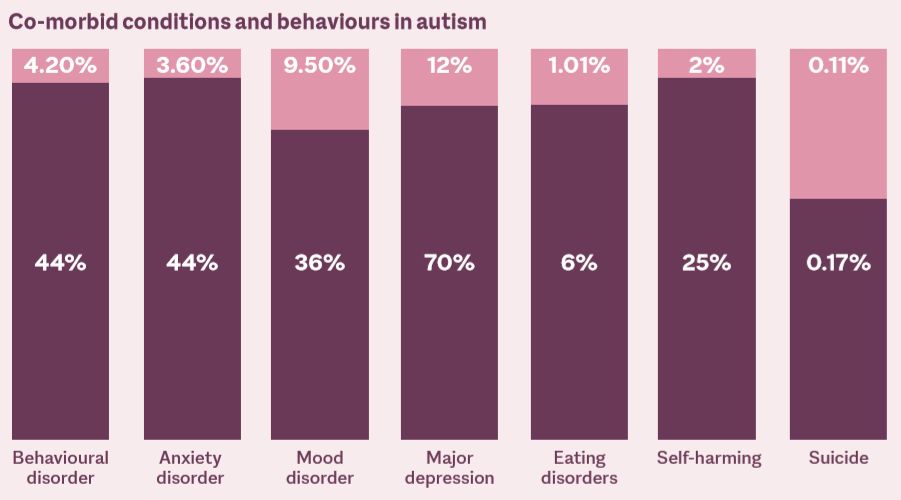
The rates of co-morbid mental health conditions are significantly higher in autistic people. In another study, autistic people have been found to be 7.55 times more likely to die by suicide, and have an average lifespan of 54 years.2 In my own lifetime, that figure is 12 years away. This study highlights another significant difference when comparing the two populations. In the general population, more men lose their lives to suicide than women, whereas conversely within the autistic population, women are more likely to lose their lives to suicide than men.2 As figure 1 shows, 70% of autistic people will suffer from depression,1 much more than the 12% in the neurotypical population. However, autistic people are less likely to be diagnosed with depression or have adequate support networks in place. This increases the risk of them losing their lives to suicide.2 When intersectionality is considered, life chances are lowered even further. For example, black, Asian and minority ethnic (BAME) autistic people are less likely to be diagnosed as autistic and will further miss out on the minimal support systems available.3
Next in this issue
There is an alarming clue behind these high depression and suicide rates. Autistic people who are better camouflaged within the neurotypical population – ie who are able to ‘act’ neurotypical, hide their autistic traits and blend in – are more likely to suffer from depression4 and are at higher risk of suicide than autistic people who choose not to, or are less able to camouflage or mask their traits.5 This is where society plays an important part in improving the quality of life of the autistic population. Reducing stigma and encouraging a positive autism identity6 are the keys to positive change. This seems obvious when you look at this issue through the lens of most counselling theories. We are taught that supporting clients to become their most authentic selves is vitally important. However, autistic people often learn to do the opposite to survive in a world where we are a minority and different from 98% of people.7
A different brain
The neurodiversity movement, a civil rights, social movement, comparable to the LGBT movement, has helped reframe how autistic people are viewed. It recognises autism as a subset of biodiversity in the human species, and it is helping to dispel the perception of autism as a medical disability with deficits and to evolve. It encourages acceptance of autistic people and their traits, rather than trying to alter them to fit better into society. It recognises the damage caused by hiding/ masking the autistic self.8,9
Autistic brains are wired differently to neurotypical brains. Studies using brain scans have discovered that in the autistic brain, there is underconnectivity on a global scale between the key cortical areas of the brain.
This is thought to cause the differences seen, which are used to diagnose autism, such as social cognition, language, executive function and sensory sensitivities.
In the neurotypical brain, these cortical areas work more seamlessly together. What this means for the autistic brain is that compensation is required. The brain of the autistic person has been found to have overconnectivity on a local scale, which is thought to overcome the global challenges.
For example, autistic people often have strengths in their visual memory.10 Brain scans have discovered a link between reasoning, general intelligence and visual processing skills completely unique to autistic people.11 Stephen Wiltshire MBE is an inspiring example of these unique abilities. He can draw fantastic cityscapes from a brief glance.
Understanding this brain difference can not only identify strengths, but also the reason behind challenges. Many autistic people struggle to maintain eye contact. This may not be for the same reason as a neurotypical person, ie due to shyness or perhaps because a person is lying. In autistic brain scans, eye contact has been found to cause a stress reaction.12 My memories as a child are filled with grown-ups around me saying, ‘Look at me when I’m talking to you!’ Like many autistic people, eye contact is not natural for me and takes a lot of concentration to maintain. As a client in counselling, I would rather concentrate on my worries than keep up with social expectations and maintain eye contact for the benefit of my counsellor. Because, when an autistic person maintains eye contact, it is often solely so that the other person feels comfortable. We often do not receive the same messages through it that neurotypical people do. Gently letting an autistic client know that eye contact is not expected can make a wonderful difference to their counselling experience, freeing them to focus on what really matters.
Sensory processing disorder
Nine out of 10 autistic people will experience sensory processing disorder. They can either be over- or under-responsive to sensory stimuli, or a mixture of both.10 Under-sensitivity can be dangerous, as a person may not feel pain or heat and could get into a bath that is too hot, or not know a bone is broken. In over-sensitivity, sounds, touch, smells and taste can be experienced as painful or intolerable. The world is louder and brighter. In busy places, we can feel overwhelmed by the sights, sounds and smells that our brains are trying to process all at once. Even in seemingly quiet places, the ticking of a clock or the whirr of a computer can drive us to distraction. An autistic person is likely to use more energy to process sensory experiences that neurotypical people often take for granted.
Theory of mind versus the ‘double empathy problem’
For the last few decades, theory of mind (TOM) has been seen in academic circles as the Holy Grail of explaining why we autistic people struggle to ‘fit in’ socially. It has been said that we have a deficit in our TOM. TOM describes the ability of people to know or predict how others think, feel, their beliefs and how they might behave. Uta Frith believes that this ability to ‘mind read’ and attribute mental states to others does not come from ‘complex logical inference’ but instead ‘…rests on a dedicated neurocognitive mechanism’.13 This is said to be delayed during development in autistic people. However, this theory also acknowledges that autistic people can develop this ability through compensatory learning, but can be error prone in more complex social situations, and struggle with things like sarcasm, for example, and when people are not saying what they mean.13
However, let’s turn the world upside down for a moment, and look at this firstly through the neurodiversity paradigm mentioned earlier, whereby autistic people are actually a different neurotype in the vast diversity of human existence, rather than thinking of us as deficit or lesser versions of the neurotypical or neuro-majority type. Then, secondly, through a theory developed by Damian Milton, known as the ‘double empathy problem’.14 This theory recognises that as much as autistic people may struggle to understand the minds and cultures of neurotypical/non-autistic people, conversely neurotypical people can struggle to understand the minds and cultures of autistic people.14 The difference is that as a ‘neurominority’, our survival depends on being able to understand the non-autistic society, which makes up the ‘neuro-majority’.9 I ask you for a moment to imagine the world upside down. It now contains 98% of autistic people, and non-autistic people are the minority. How does it feel? What will you need to do to survive? Can you be your real self and still ‘fit in’?
Conditions of worth
Life teaches us to mask our autistic traits to ‘fit in’ and appear indistinguishable from our neurotypical peers. We do this to avoid bullying. Autistic children are bullied twice as much as their neurotypical peers.15 We keep our intense interests to ourselves because we fear or experience that others are not interested in them. We hide our extreme sensory discomfort in busy environments where our peers appear at ease. We try to not let on that we have misunderstood some important social cues, or that we have been misunderstood. We maintain eye contact when it makes us deeply uncomfortable. We suppress stims (self-stimulating behaviours used to soothe intense emotions)16 so as not to stand out. We mask to feel safe and accepted. We place a condition of worth on being able to do all of this. We hide the fact that all these struggles drain our energy levels and can lead to autistic burnout, anxiety and depression. Research tells us that this masking behaviour can increase the risk of suicide, and the more ‘successful’ we are at acting neurotypical, the more at risk we are of suicide.5
Counselling autistic clients
Counselling can be the first time that we experience a relationship where we are truly accepted, so please provide that acceptance by being knowledgeable about autism and providing an environment with a relationship that we can reach. I end this article with a table with practical tips, detailing how you can adapt in specific areas to help provide a positive counselling experience and influence positive autistic identity.
Related articles
References
1 Cromar L. A literature review exploring the efficacy of person-centred counselling for autistic people. In: Milton D (ed). The neurodiversity reader (1st edition). Pavilion Publishing and Media Ltd; 2020.
2 Hirvikoski T, Mittendorfer-Rutz E, Boman M, Larsson H, Lichtenstein P, Bölte S. Premature mortality in autism spectrum disorder. British Journal of Psychiatry 2016; 208(3): 232–238.
3 Slade G. Diverse perspectives. London: National Autistic Society; 2014.
4 Cage E, Di Monaco J, Newell V. Experiences of autism acceptance and mental health in autistic adults. Journal of Autism and Developmental Disorders 2017; 48(2): 473–484. 5 Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Molecular Autism 2018; 9(1). https://doi.org/10.1186/ s13229-018-0226-4.
6 Cooper K, Smith L, Russell A. Social identity, self-esteem, and mental health in autism. European Journal of Social Psychology 2017; 47(7): 844–854.
7 Centers for Disease Control and Prevention. Data and statistics on autism spectrum disorder. [Online.] https://www.cdc.gov/ncbddd/autism/ data.html (accessed 3 October 2020).
8 Singer J. Neurodiversity: the birth of an idea. Judy Singer; 2017.
9 Singer J. Neurodiversity 2.0: what is neurodiversity? [Online.] https://neurodiversity2.blogspot.com/p/ what.html (accessed 4 October 2020).
10 Grandin T, Panek R. The autistic brain. London: Random House; 2013.
11 Soulières I, Zeffiro T, Girard M, Mottron L. Enhanced mental image mapping in autism. Neuropsychologia 2010; 49(5): 848–857.
12 Hadjikhani N, Åsberg Johnels J, Zürcher N, Lassalle A, Guillon Q, Hippolyte L et al. Look me in the eyes: constraining gaze in the eye-region provokes abnormally high subcortical activation in autism. Scientific Reports 2017; 7(1). https://doi. org/10.1038/s41598-017-03378-5
13 Frith U. Mind blindness and the brain in autism. Neuron 2001; 32: 969–979.
14 Milton D. On the ontological status of autism: the ‘double empathy problem’. Disability & Society 2012; 27(6): 883–887.
15 Cappadocia M, Weiss J, Pepler D. Bullying experiences among children and youth with autism spectrum disorders. Journal of Autism and Developmental Disorders 2011; 42(2): 266–277.
16 Kapp S, Steward R, Crane L, Elliott D, Elphick C, Pellicano E et al. ‘People should be allowed to do what they like’: autistic adults’ views and experiences of stimming. Autism 2019; 23(7): 1782–1792.